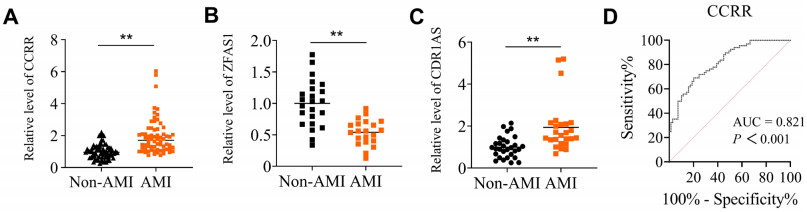
| Citation: | Lina Xuan, Huishan Luo, Shu Wang, Guangze Wang, Xingmei Yang, Jun Chen, Jianjun Guo, Xiaomeng Duan, Xiufang Li, Hua Yang, Shengjie Wang, Hailong Zhang, Qingqing Zhang, Shulei Liu, Yongtao She, Kai Kang, Lihua Sun. Circulating CCRR serves as potential novel biomarker for predicting acute myocardial infarction[J]. Frigid Zone Medicine, 2024, 4(3): 137-151. doi: 10.1515/fzm-2024-0015

|

| [1] |
Roth G A, Mensah G A, Johnson C O, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J. Am. Coll. Cardiol, 2020; 76: 2982-3021.
|
| [2] |
Liu S, Li Y, Zeng X, et al. Burden of cardiovascular diseases in China, 1990-2016: findings from the 2016 global burden of disease study. JAMA Cardiology, 2019; 4 (4): 342-352. doi: 10.1001/jamacardio.2019.0295
|
| [3] |
Zhao D. Epidemiological features of cardiovascular disease in Asia. JACC: Asia, 2021; 1 (1): 1-13. doi: 10.1016/j.jacasi.2021.04.007
|
| [4] |
Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: a nationwide population-based cohort study. The Lancet Public Health, 2020; 5 (12): e672-e681. doi: 10.1016/S2468-2667(20)30191-2
|
| [5] |
Lei J, Chen R, Yin P, et al. Association between cold spells and mortality risk and burden: a nationwide study in China. Environmental Health Perspectives, 2022; 130 (2): 027006. doi: 10.1289/EHP9284
|
| [6] |
Schulte C, Barwari T, Joshi A, et al. Noncoding RNAs versus protein biomarkers in cardiovascular disease. Trends Mol Med, 2020; 26: 583-596. doi: 10.1016/j.molmed.2020.02.001
|
| [7] |
Emdin M, Aimo A, Vergaro G, et al. sST2 predicts outcome in chronic heart failure beyond NT-proBNP and high-sensitivity troponin T. J Am Coll Cardiol, 2018; 72: 2309-2320. doi: 10.1016/j.jacc.2018.08.2165
|
| [8] |
Wang Y, Sun X. The functions of LncRNA in the heart. Diabetes Res Clin Pract, 2020; 168: 108249. doi: 10.1016/j.diabres.2020.108249
|
| [9] |
Mozaffarian D, Benjamin E J, Go A S, et al. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation, 2015; 131: e29-322. doi: 10.1161/circ.131.suppl_2.o29
|
| [10] |
Kopp F, Mendell J T. Functional classification and experimental dissection of long noncoding RNAs. Cell, 2018; 172: 393-407. doi: 10.1016/j.cell.2018.01.011
|
| [11] |
Chang G, Zhang W, Zhang M, et al. Clinical value of circulating ZFAS1 and miR-590-3p in the diagnosis and prognosis of chronic heart failure. Cardiovasc. Toxicol, 2021; 21: 880-888. doi: 10.1007/s12012-021-09678-7
|
| [12] |
Sharma S, Findlay G M, Bandukwala H S, et al. Dephosphorylation of the nuclear factor of activated T cells (NFAT) transcription factor is regulated by an RNA protein scaffold complex. Proc Natl Acad Sc, 2011; 108: 11381-11386. doi: 10.1073/pnas.1019711108
|
| [13] |
Viereck J, Thum T. Circulating noncoding RNAs as biomarkers of cardiovascular disease and injury. Circ Res, 2017; 120: 381-399. doi: 10.1161/CIRCRESAHA.116.308434
|
| [14] |
Cao M, Luo H, Li D, et al. Research advances on circulating long noncoding RNAs as biomarkers of cardiovascular diseases. Int J Cardiol, 2022; 353: 109-117. doi: 10.1016/j.ijcard.2022.01.070
|
| [15] |
Zhang Y, Sun L, Xuan L, et al. Reciprocal changes of circulating long non-coding RNAs ZFAS1 and CDR1AS predict acute myocardial infarction. Sci Rep, 2016; 6: 2384.
|
| [16] |
Wang X, Wang L, Ma Z, et al. Early expressed circulating long noncoding RNA CHAST is associated with cardiac contractile function in patients with acute myocardial infarction. Int J Cardiol, 2020; 302: 15-20. doi: 10.1016/j.ijcard.2019.12.058
|
| [17] |
Tang Y, Zheng J, Sun Y, et al. MicroRNA-1 regulates cardiomyocyte apoptosis by targeting Bcl-2. Int Heart J, 2009; 50: 377-387. doi: 10.1536/ihj.50.377
|
| [18] |
Gao L, Liu Y, Guo S, et al. Circulating long noncoding RNA HOTAIR is an essential mediator of acute myocardial infarction. Cell. Physiol. Biochem, 2017; 44: 1497-1508. doi: 10.1159/000485588
|
| [19] |
Azat M, Huojiahemaiti X, Gao R, et al. Long noncoding RNA MIAT: a potential role in the diagnosis and mediation of acute myocardial infarction. Mol Med Rep, 2019; 20: 5216-5222.
|
| [20] |
Wang L, Wang L, Wang Q. Constitutive activation of the NEAT1/miR-22-3p/Ltb4r1 signaling pathway in mice with myocardial injury following acute myocardial infarction. Aging (Albany NY), 2021; 13: 15307-15319.
|
| [21] |
Li M, Wang Y F, Yang X C, et al. Circulating long noncoding RNA LIPCAR acts as a novel biomarker in patients with ST-segment elevation myocardial infarction. Med Sci Monit, 2018; 24: 5064-5070. doi: 10.12659/MSM.909348
|
| [22] |
Yan L, Zhang Y, Zhang W, et al. lncRNA-NRF is a potential biomarker of heart failure after acute myocardial infarction. J Cardiovasc Transl Res, 2020; 13: 1008-1015. doi: 10.1007/s12265-020-10029-0
|
| [23] |
Zhang Y, Sun L, Xuan L, et al. Long non-coding RNA CCRR controls cardiac conduction via regulating intercellular coupling. Nat Commun, 2018; 9: 4176. doi: 10.1038/s41467-018-06637-9
|
| [24] |
Khodayi M, Khalaj-Kondori M, Hoseinpour F M A, et al. Plasma lncRNA profiling identified BC200 and NEAT1 lncRNAs as potential blood-based biomarkers for late-onset Alzheimer's disease. EXCLI J, 2022; 21: 772-785.
|
| [25] |
Isaac R, Reis F C G, Ying W, et al. Exosomes as mediators of intercellular crosstalk in metabolism. Cell Metab, 2021; 33: 1744-1762. doi: 10.1016/j.cmet.2021.08.006
|
| [26] |
Zheng M L, Liu X Y, Han R J, et al. Circulating exosomal long noncoding RNAs in patients with acute myocardial infarction. J Cell Mol Med, 2020; 24: 9388-9396. doi: 10.1111/jcmm.15589
|
| [27] |
Catalano M, O'Driscoll L. Inhibiting extracellular vesicles formation and release: a review of EV inhibitors. J Extracell Vesicles, 2020; 9, 1703244. doi: 10.1080/20013078.2019.1703244
|
| [28] |
Crea F. How epidemiology can improve the understanding of cardiovascular disease: from mechanisms to treatment. Eur Heart J, 2021; 42: 4503-4507. doi: 10.1093/eurheartj/ehab797
|
| [29] |
Lerman B, Lerman L O. "Nothing burns like the cold": Cardiovascular disease in frigid zones. Frigid Zone Medicine, 2022; 2 (3): 129-131. doi: 10.2478/fzm-2022-0017
|
| [30] |
Jin H. Increased risk of cardiovascular disease in cold temperatures. Frigid Zone Medicine, 2022; 2 (3): 138-139. doi: 10.2478/fzm-2022-0020
|
| [31] |
Oitabén A, Fonseca P, Villanueva M J, et al. Emerging blood-based biomarkers for predicting immunotherapy response in NSCLC. Cancers (Basel), 2022; 14 (11), 2626. doi: 10.3390/cancers14112626
|
| [32] |
Chaitman B R, Cyr D D, Alexander K P, et al. Cardiovascular and renal implications of myocardial infarction in the ISCHEMIA-CKD trial. Circ Cardiovasc Interv, 2022; 15: e012103.
|
| [33] |
Wang F, Li X, Xie X, et al. UCA1, a non-protein-coding RNA upregulated in bladder carcinoma and embryo, influencing cell growth and promoting invasion. FEBS Lett, 2008; 582: 1919-1927. doi: 10.1016/j.febslet.2008.05.012
|
| [34] |
Yan Y, Zhang B, Liu N, et al. Circulating long noncoding RNA UCA1 as a novel biomarker of acute myocardial infarction. Biomed Res Int, 2016; 2016: 8079372.
|
| [35] |
Zheng P F, Chen L Z, Liu P, et al. A novel lncRNA-miRNA-mRNA triple network identifies lncRNA XIST as a biomarker for acute myocardial infarction. Aging (Albany NY), 2022; 14: 4085-4106.
|
| [36] |
Wang Y, Zhao R, Liu W, et al. Exosomal circHIPK3 released from hypoxia-pretreated cardiomyocytes regulates oxidative damage in cardiac microvascular endothelial cells via the miR-29a/IGF-1 pathway. Oxid Med Cell Longev, 2019; 2019: 7954657.
|
| [37] |
Gupta S, Knowlton A A. HSP60 trafficking in adult cardiac myocytes: role of the exosomal pathway. Am J Physiol Heart Circ Physiol, 2007; 292: H3052-3056.
|
| [38] |
King H W, Michael M Z, Gleadle J M. Hypoxic enhancement of exosome release by breast cancer cells. BMC Cancer, 2021; 12: 421.
|
| [39] |
Vicencio J M, Yellon D M, Sivaraman V, et al. Plasma exosomes protect the myocardium from ischemia-reperfusion injury. J Am Coll Cardiol, 2015; 65 (15): 1525-1536.
|
| [40] |
Tomasoni S, Longaretti L, Rota C, et al. Transfer of growth factor receptor mRNA via exosomes unravels the regenerative effect of mesenchymal stem cells. Stem Cells Dev, 2013; 22 (5): 772-778.
|
| [41] |
Jiao L, Li M, Shao Y, et al. lncRNA-ZFAS1 induces mitochondriamediated apoptosis by causing cytosolic Ca2+ overload in myocardial infarction mice model. Cell Death Dis, 2019; 10: 942.
|
| [42] |
Shao Y, Li M, Yu Q, et al. CircRNA CDR1as promotes cardiomyocyte apoptosis through activating hippo signaling pathway in diabetic cardiomyopathy. Eur J Pharmacol, 2022; 922: 174915.
|
Figures(7) / Tables(4)
Editorial Office: Frigid Zone Medicine, Editorial Office of Frigid Zone Medicine, Heilongjiang Health Development Research Center, Zhongshan Road 112, Xiangfang District, Harbin, 150036, China
Tel: 0451-87253028
E-mail: editorialoffice@frigidzonemedicine.com
Supported by:
Beijing Renhe Information Technology Co., Ltd.


 Submit
Submit


 DownLoad:
DownLoad: